
7/11/2024

Earlier this month, the Federal Trade Commission (FTC) published an interim report about the “powerful middlemen” of the pharma industry: Pharmacy Benefit Managers or PBMs. You can find the FTC’s summary as well as the full report on their website.
After reading the report, I am generally aligned with the overall finding from the commission that "underscores the impact pharmacy benefit managers have on the accessibility and affordability of prescription drugs." It only takes a quick Google search of the Fortune 500 to see how many PBMs rank in the top 25: United Health (#4), CVS Caremark (#6), Cigna (#16) and Centene (#22). You may also note that in addition to the PBMs, McKesson (#9), Cencora (#10) and Cardinal Health (#14) are all listed much higher than the first pharmaceutical company, Johnson & Johnson (#42). Despite this, public perception is that pharmaceutical manufacturers are at fault for high drug prices... Curious isn't it?
I'm digressing a bit, but this is key to what most of us in the industry have known for years — that there are numerous companies generating their revenues from pharmaceutical manufacturers while escaping any kind of scrutiny for their role in drug pricing. Hopefully, this report, and the on-going inquiry, will help the public better understand the complexities and drivers of the pharmaceutical market. Here are my three takeaways from the report.
First, the FTC did an admirable job of capturing and visualizing the vertical integration that had occurred within PBMs. Figure 1 of the report and Figure 3 present a clear picture of the vertical integration, which is the first step in understanding the control and influence PBMs wield on the pharma channel and, ultimately, the patients.
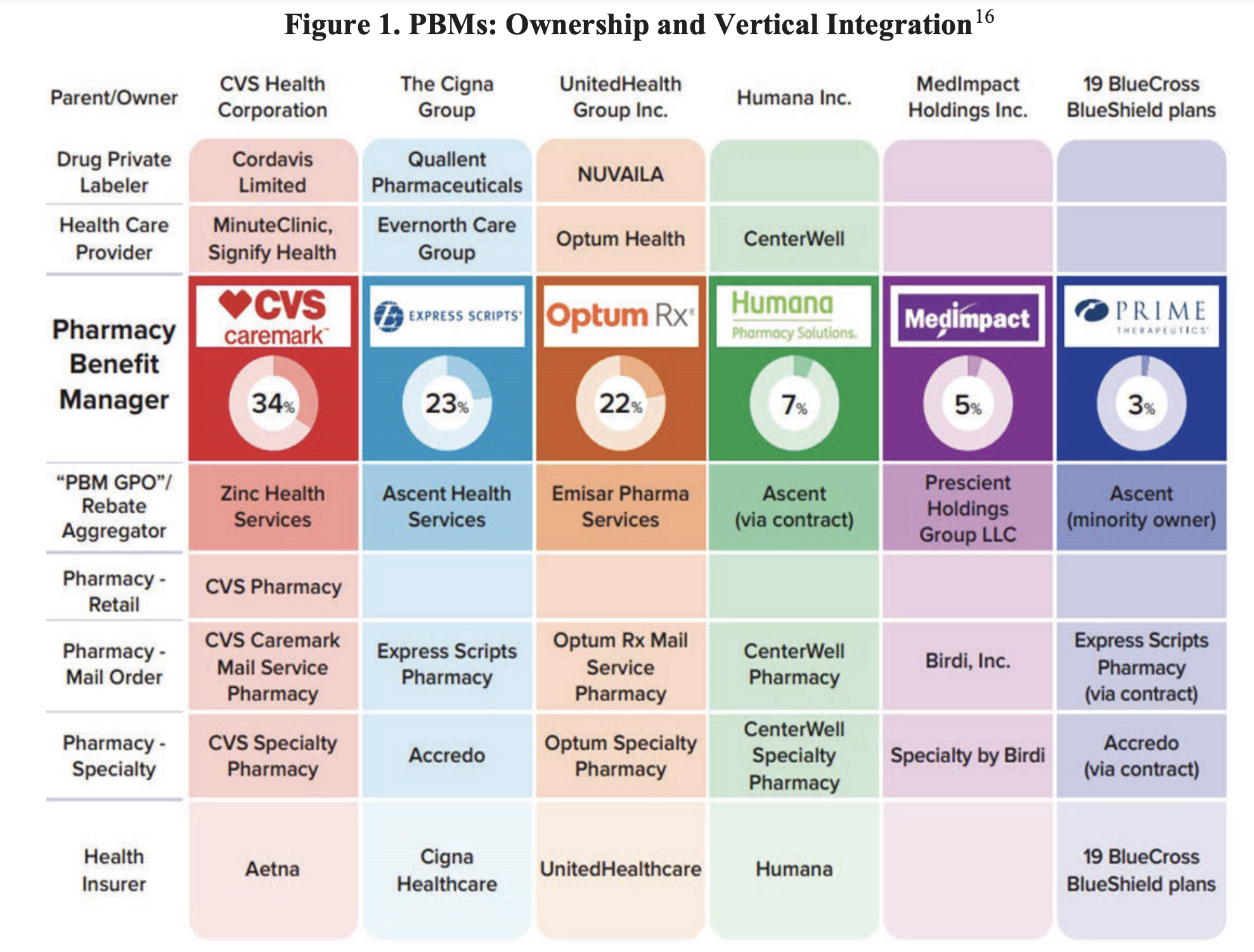
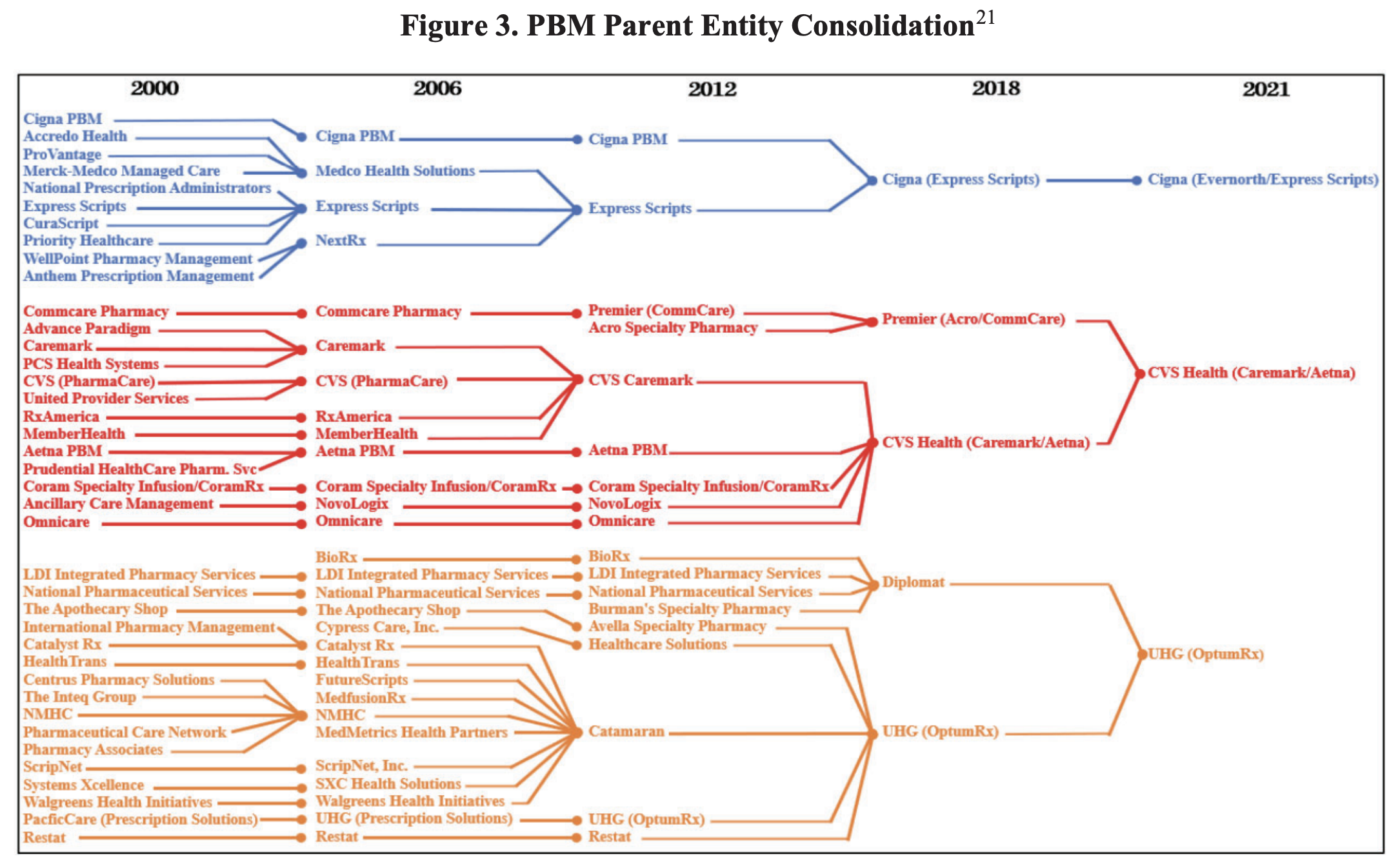
According to their analysis, "increasing vertical integration and concentration has enabled the six largest PBMs to manage nearly 95 percent of all prescriptions filled in the United States." While you can tell from the report that the FTC are not fully attuned to the nuances of drug distribution, they did get the overall picture right. When any entity owns so many supply chain touchpoints between the manufacturer and the patient, it enjoys numerous opportunities to profit at the expense of both the manufacturer and the patient.
My second observation was the FTC highlighting the relationship of the PBM and the pharmacies. This relationship is so key in the patient's experience that it cannot be overlooked when evaluating the PBM's role. They are not only controlling the patient's access to obtaining product through insurance, they are directly influencing which product the patient has access to when they actually fill the prescription. This gives the PBM multiple opportunities to favor drugs that make the PBM the most money, not the drugs that are best therapeutically or cheapest for the patient. The layers of PBM interference range from controlling pharmacy reimbursement rates to overall product availability to suppressing independent pharmacy competition.
My last observation was the dissenting statement by Commissioner Melissa Holyoak, which generally asserts that the interim report was not conducted with the FTC's typical meticulous protocol. Her comments seem to be missing the point of why the report was issued, and serve as a distraction. A major reason the FTC issued the interim report was that PBMs had not been forthcoming or timely in their responses to the commission's requests for information. Instead of acknowledging this, the commissioner primarily dissented due to the lack of acknowledgment of the FTC's previous 2005 PBM report that focused on the ownership of mail-order pharmacies and the "standards of economic rigor expected" from the commission. Commissioner Holyoak seems so focused on the 2005 report and protocol precedents that it colors her perspective on the market almost 20 years later. As anyone currently working in market access can tell you, the demands on pharmaceutical manufacturers are fundamentally different today than even 5 years ago... let alone 20. I am concerned that a commissioner of a government entity with large potential influence on industry regulation cannot see the proverbial forest for the trees.
To be clear, I do not think Commissioner Holyoak is advocating for PBMs. I just believe that her focus is misplaced and will ultimately distract from the regulatory changes that are needed to ensure that manufacturers can continue developing life saving medications for the people. With all of the government regulations impacting manufacturers that have been implemented, as well as those that are proposed (e.g. HR 1319, the Inflation Reduction Act, etc.), we need Congress to be able to cut to the core issue and not be distracted on outdated references and minutiae.
There is a large amount of very good information in the report, and I highly recommend that anyone in a market access role take the time to dig into it and compare it to your experiences with your products. As always, if you are interested in discussing any of the details of the report or question you may have, please reach out.
Recent Articles
Physician Fee Schedule FAQ and Templates
CMS published its FAQ on Bona Fide Service Fee Certifications and ASP Reasonable Assumptions.
2026 GP Calendar
Key Government Pricing dates for 2026 to add to your Outlook or Google Calendar.

MDRP 2025 Wrap-up
Salient topics and key takeaways from the MDRP 2025 conference.
View All News & Opinions
Talk to an Expert
Get Started%20(1).avif)
.avif)